Since it was enacted, President Obama has used all manners of executive power to salvage the Affordable Care Act–at least in the short term. (Many of his exemptions and waivers to the waivers inflicted long-term structural damage to the marketplaces). Now, in his first day of office, President Trump has embarked on using the same species of power to undo Obamacare. Hours after taking the oath of office, President Trump signed an executive order to “minimiz[e] the economic burden of” the ACA.
Signing documents to allow Mattis and Kelly to be sworn into Cabinet and an executive order on #Obamacare. https://t.co/zg3WP9w8xC pic.twitter.com/OMOGLTkCDA
— President Trump (@POTUS) January 21, 2017
Section 1 of the Order states that “it is the policy of my Administration to seek the prompt repeal” of the ACA. There is no doubt or walking back this line. Further,
“it is imperative for the executive branch to ensure that the law is being efficiently implemented, take all actions consistent with law to minimize the unwarranted economic and regulatory burdens of the Act, and prepare to afford the States more flexibility and control to create a more free and open healthcare market.
How will this be accomplished? Section 2 states that the Secretary of HHS, and other officials,
“shall exercise all authority and discretion available to them to waive, defer, grant exemptions from, or delay the implementation of any provision or requirement of the Act that would impose a fiscal burden on any State or a cost, fee, tax, penalty or regulatory burden on individuals, families, healthcare providers, health insurers, patients, recipients of healthcare services, purchasers of health insurance, or makers of medical devices, products, or medications.”
There is, of course one proviso: HHS can only act here “to the maximum permitted by law.” What is that extent? Under the precedents of the Obama administration, there are no meaningful bounds. Secretary Sebelius deemed it a hardship if anyone had difficulty affording insurance under the ACA, permitting a waiver of the individual mandate. (As Ezra Klein famously put it, “Obamacare itself is the hardship”). Trump’s order follows a similar pattern. If the Obamacare “tax” (thank you John Roberts) imposes a “burden” on individuals, the Secretary now has the authority to defer the mandate.
This discretion is not limited to states. Secretary Sebelius also permitted states to suspend enforcement of “minimum essential coverage,” and allow the sale of non-compliant policies, citing the unfairness of people whose plans would otherwise be cancelled. Thus, if “minimum essential coverage” impose a “fiscal burden on any state,” the Secretary can now suspend it. Using all of the precedents developed by the Obama administration, Trump can now take systematic steps to unravel Obamacare. (Note that I’ve written at length that all of these actions were illegal, and will be illegal).
Perhaps the most important provision is Section 5.
“To the extent that carrying out the directives in this order would require revision of regulations issued through notice-and-comment rule-making, the heads of agencies shall comply with the Administrative Procedure Act and other applicable statues in considering or promulgating such regulatory revisions.”
The order, by itself, takes no action. It merely signals to his administration what his priorities are. But the impact is unmistakeable. The Secretaries of the various departments will take the direction, issue memorandums, rescind memorandums, and rescind rules.
At the moment, the “Executive Order” page of WhiteHouse.gov is blank. Expect this page to be filled up as the days go by.
![]()
Update: On cue, ardent defenders of President Obama’s executive actions have now discovered the separation of powers:
But this executive action on its own does not unravel the mandate on its own, or any other part of Obamacare for that matter. Instead, it sets up a long, drawn-out process to change the law’s rules — a unwinding process that takes time. And there are still major limits to how much Trump can do before Congress acts.
“Trump is going to have to comply with law, and that doesn’t allow him to repeal the Affordable Care Act unilaterally,” health law expert Tim Jost, a law professor at Washington and Lee College, says.
As the above post notes, the precedents of the administrative fix, and the hardship exemptions, provides a broad basis to suspend “minimum essential coverage” requirements as well as the individual mandate.
Update 2: Nick Bagley reads the EO in much the same way with respect to killing the individual mandate–a step that would be illegal, but entirely consistent with Secretary Sebelius’s decision.
What troubles me most is the instruction to “delay the implementation of” any “tax” on individuals. Back in 2013, the Obama administration delayed the implementation of both the employer mandate and some of the ACA’s insurance rules. The implementation delays were unlawful, as I argued at the time. I warned, too, that they were shortsighted:
A future administration that is less sympathetic to the ACA could invoke the delays as precedent for declining to enforce other provisions that it dislikes, including provisions that are essential to the proper functioning of the law. The delays could therefore undermine the very statute they were meant to protect—and perhaps imperil the ACA’s effort to extend coverage to tens of millions of people.
Delaying the individual mandate is precisely what I feared most. (The E.O.’s instruction to consider delaying implementation of taxes on “makers of medical devices, products, or medications” could also lead to the suspension of the medical device tax and the tax on the pharmaceutical industry. That’d be a sweetheart gift for industry.)
Update 3: Seth Chandler reaches much the same conclusion:
1. “Delay” enforcement of the individual and employer mandates. President Obama, after all, delayed enforcement of the employer mandate for a year for some large employers and delayed enforcement for two years for others. It was, the President asserted, too burdensome to comply with. President Trump might equally assert that, given the poor quality and high prices of ACA policies in many jurisdictions, it is too burdensome to comply with the individual mandate today. And the employer mandate, with its exacting employee-counting rules, remains somewhat burdensome. Moreover, even if there are differences in kind and degree between President Obama’s actions and those taken pursuant to the Trump Executive Order, who would have standing to challenge any lack of enforcement? It’s all part of the “discretion” on which the Obama administration rested many actions under the ACA and other statutes. And it will take some work for Obama supporters to object to actions by the Trump administration to engage in these “delays” since President Obama did it himself.
2. Expand “hardship exemptions” from the individual mandate so that basically nobody has to pay what many conservatives still regard as an unconstitutional tax. President Obama, after all, without notice and comment created hardship exemptions that had, quite arguably, little to do with actual hardship and a lot to do with politics: the exemption of persons who can afford insurance but who live in a state that dared not to expand Medicaid would be my Exhibit A on this point. And, again, even if granting such a hardship were unlawful, at least without notice and comment rule making, who is going to have standing to challenge the “enforcement priority?” Either delay of the individual mandate or expansion of the hardship exemption would threaten continued participation of insurers selling policies on the individual market.
3. Extend the option of the states to permit insurers to sell insurance policies that do not comply with ACA requirements regarding matters such as “benefit packages” (maternity, contraceptives, pre-existing condition limits, etc). Such sales would make Exchange policies less attractive to many men, younger persons or others who want policies that are cheaper (and often provide less coverage) then those sold on the Exchanges. How could President Trump do this lawfully or without sluggish notice and comment rule making? The same way President Obama did in November of 2013 — by executive order and a regulatory guidance! Remember the firestorm of protest when it was discovered that President Obama had issued the “lie of the year” when he said that if you liked your healthcare plan you could keep your healthcare plan. Period. The “Administrative Fix” explicitly permitted states to let their insurers violate the ACA, an invitation that was accepted by some jurisdictions and rejected by others. Oh, and think that surely a court would overturn such a subversion of the law by decree? Ask West Virginia. Its case objecting to this apparent abuse of separation of powers was tossed out by the United States Court of Appeals for the District of Columbia. Maybe the Supreme Court will ultimately overturn the Court of Appeals, but, even if so, it will have taken West Virginia more than three years to restore the rule of law.
Tim Jost, on the other hand, now asserts there are limits on what can be a “hardship”:
New categories of hardship exemptions to the individual responsibility requirement may be created, but they will have to qualify as hardships. …
A number of commenters have noted that the Order seems to instruct HHS to liberally grant waivers from the individual responsibility requirement of the ACA. The ACA gives HHS discretion in granting “hardship” waivers and current regulations authorize HHS to do this through guidance. The Obama administration authorized hardship waivers in a number of circumstances, and one can imagine Trump’s HHS granting hardship exemptions even more broadly, perhaps even through guidance.
But surely the term “hardship” is not meaningless—simply being required to purchase health insurance is not in itself a hardship, because that is what the individual responsibility law requires. Were the Trump administration to effectively repeal the mandate, it would certainly be sued. Individuals with preexisting conditions left in a market without healthy enrollees would have a strong argument for standing. Also, as the Congressional Budget Office has acknowledged, repealing the individual responsibility requirement could have a devastating effect on the individual insurance market if it is not replaced by another means of encouraging healthy people to enroll. Would the Trump administration want to risk destroying the individual market through executive action? We will see.
Oh but under Secretary Sebelius’s standards, “hardship” is meaningless. From Unraveled:
The legal basis for the hardship fix was sketched out by Professors Nicholas Bagley and Austin Frakt two months earlier, in an article aptly titled “Saving Obamacare without Congress.” 113 First, the professors explained that the law allows for a “hardship exemption” for anyone who has “suffered “suffered a hardship with respect to the capability to obtain coverage under a qualified health plan.” Second, they wrote, Secretary Sebelius can “grant a certification” for particular individuals attesting that “there is no affordable qualified health plan available through the Exchange.” As a result, if these two provisions are put together, the scholars explained, it could be a “hardship” if there was “no affordable qualified health plan available through the Exchange.”
But there is an ironic quality to this reasoning. Congress created several categories of people who would be exempted from the individual mandate’s penalty: “individuals who cannot afford coverage,” “taxpayers with incomes below filing threshold,” “member[ s] of Indian tribes,” and anyone who “suffered a hardship with respect to the capability to obtain coverage under a qualified plan.” 114 Congress set a strict threshold for exemptions from the penalty due to inability to pay: those for whom the annual cost of coverage exceeds 8 percent of household income. 115 These are individuals with extremely low incomes, who would likely qualify for Medicaid.
HHS’s blanket policy of exempting anyone whose insurance was “more expensive” than before, irrespective of annual income, is impossible to reconcile with the congressional scheme. This hardship “exemption” swallows the rule. Ezra Klein aptly summarized the change: “In other words, Obamacare itself is the hardship.” 116 University of Houston Law professor Seth Chandler joked, “Surely, however, the existence of the ACA itself cannot be the human-caused event creating the hardship.” 117 Through this administrative-law shell game, the executive swept away Congress’s exemption design. The Wall Street Journal editorialized, “A tornado destroys the neighborhood or ObamaCare blows up the individual insurance market, what’s the difference?” 118
Those who defended this extremely broad reading of “hardship” in 2013 will now have to reconcile a similarly broad reading of “hardship” in 2017.
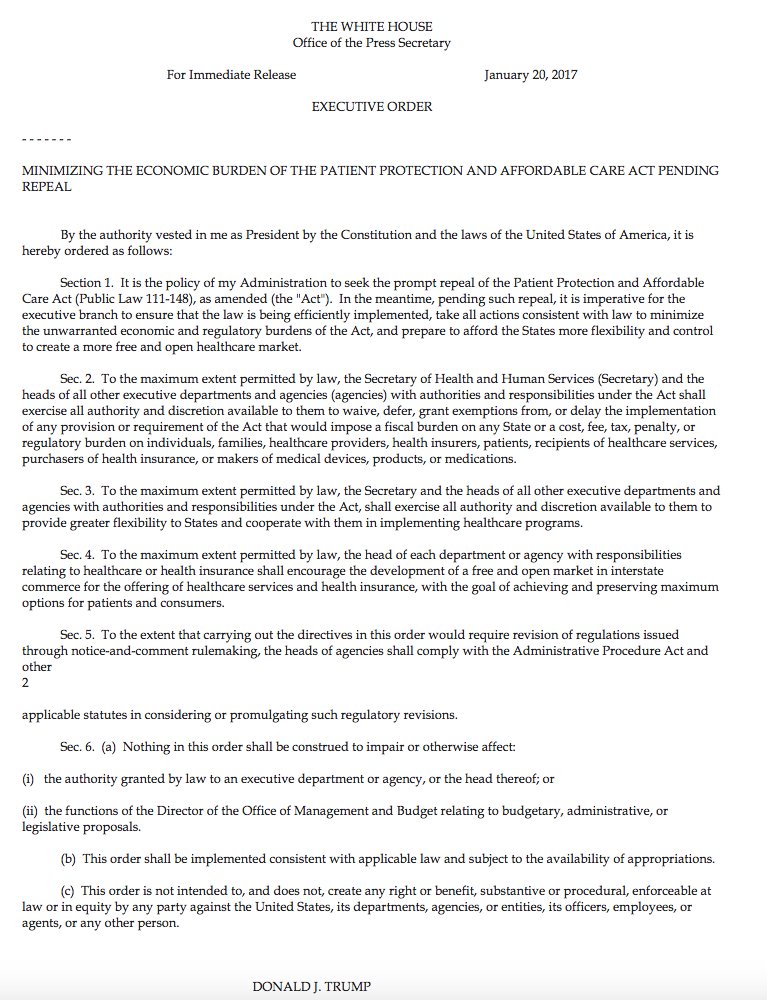
Update 4: Here is the full text of the executive order:
MINIMIZING THE ECONOMIC BURDEN OF THE PATIENT PROTECTION AND AFFORDABLE CARE ACT PENDING REPEAL
By the authority vested in me as President by the Constitution and the laws of the United States of America, it is hereby ordered as follows:
Section 1. It is the policy of my Administration to seek the prompt repeal of the Patient Protection and Affordable Care Act (Public Law 111-148), as amended (the “Act”). In the meantime, pending such repeal, it is imperative for the executive branch to ensure that the law is being efficiently implemented, take all actions consistent with law to minimize the unwarranted economic and regulatory burdens of the Act, and prepare to afford the States more flexibility and control to create a more free and open healthcare market.
Sec. 2. To the maximum extent permitted by law, the Secretary of Health and Human Services (Secretary) and the heads of all other executive departments and agencies (agencies) with authorities and responsibilities under the Act shall exercise all authority and discretion available to them to waive, defer, grant exemptions from, or delay the implementation of any provision or requirement of the Act that would impose a fiscal burden on any State or a cost, fee, tax, penalty, or regulatory burden on individuals, families, healthcare providers, health insurers, patients, recipients of healthcare services, purchasers of health insurance, or makers of medical devices, products, or medications.
Sec. 3. To the maximum extent permitted by law, the Secretary and the heads of all other executive departments and agencies with authorities and responsibilities under the Act, shall exercise all authority and discretion available to them to provide greater flexibility to States and cooperate with them in implementing healthcare programs.
Sec. 4. To the maximum extent permitted by law, the head of each department or agency with responsibilities relating to healthcare or health insurance shall encourage the development of a free and open market in interstate commerce for the offering of healthcare services and health insurance, with the goal of achieving and preserving maximum options for patients and consumers.
Sec. 5. To the extent that carrying out the directives in this order would require revision of regulations issued through notice-and-comment rulemaking, the heads of agencies shall comply with the Administrative Procedure Act and other applicable statutes in considering or promulgating such regulatory revisions.
Sec. 6. (a) Nothing in this order shall be construed to impair or otherwise affect:
(i) the authority granted by law to an executive department or agency, or the head thereof; or
(ii) the functions of the Director of the Office of Management and Budget relating to budgetary, administrative, or legislative proposals.
(b) This order shall be implemented consistent with applicable law and subject to the availability of appropriations.
(c) This order is not intended to, and does not, create any right or benefit, substantive or procedural, enforceable at law or in equity by any party against the United States, its departments, agencies, or entities, its officers, employees, or agents, or any other person.
DONALD J. TRUMP
THE WHITE HOUSE,
January 20, 2017.